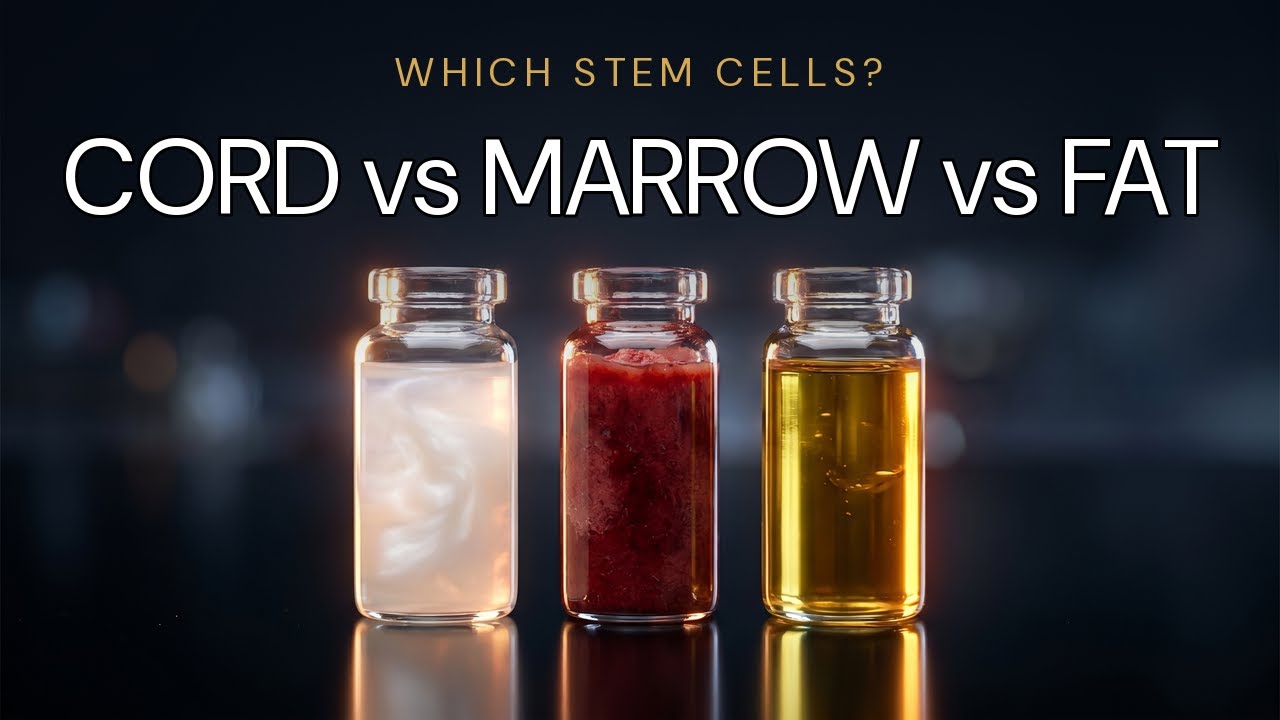
The three sources, side by side.
The three sources used in commercial regenerative medicine today are umbilical cord tissue (allogeneic, donor-derived), bone marrow (autologous, your own), and adipose tissue / fat (autologous, your own). Each has a different yield, a different cell age, a different harvest procedure, and a different track record in the clinical literature.
The marketing copy at most clinics flattens these distinctions into "stem cell therapy." The biology does not flatten them.
One label. Three very different products.
Each row is a measurable axis. Each pip is one source plotted on that axis. Where the pips cluster together, the sources are interchangeable. Where they spread, they are not.
Umbilical cord tissue. the youngest cells available.
The umbilical cord is the connective-tissue link between mother and newborn during pregnancy. After delivery, it's medical waste. With consent from the mother, the cord tissue can be donated, screened, and used as a source of mesenchymal stem cells.
Cord-derived MSCs are not embryonic. They're not from the baby. They're from the post-birth tissue that connected the placenta to the newborn, tissue that the body has finished using. Ethically, this is a non-issue: the tissue is donated with consent and would otherwise be discarded.
Why the source matters biologically
Cord MSCs are functionally newborn cells. They've existed for nine months. They have not been exposed to decades of environmental stress, accumulated mutations, or age-related decline in expansion capacity. In laboratory expansion, they double more times before senescence than marrow-derived cells from a 60-year-old donor: meaning a single donor batch can yield well over a hundred million high-quality cells, characterized and frozen, ready for clinical use.
The order-of-magnitude between sources
Cord-derived batches are produced by expansion; bone marrow and fat are typically delivered same-day without significant expansion. Y-axis is log-scaled by intent, the bars are relative.
This is the basis of standardization: every patient receives cells from the same batch, with the same characterization, the same release testing, and the same potency. Autologous sources cannot offer this.
Donor screening
Cord donation requires extensive mother and infant screening. Tested in serious programs: HIV, hepatitis B and C, syphilis, HTLV, CMV, West Nile, Zika, Chagas, and others depending on geography. The donor's medical history is reviewed. The infant's health at delivery is reviewed. The cord tissue itself is tested.
A clinic claiming to use cord-derived MSCs without being able to describe its donor screening process is a clinic that does not control its supply chain.
"What's your donor screening protocol? What pathogens are tested for? Where are the donors located, and is the donation consented and IRB-overseen?" A clinic operating a real cord-derived program can answer immediately. A clinic that purchases from outside labs may not know.
Bone marrow: autologous, low yield, age-dependent.
Bone marrow aspirate has the longest history in regenerative medicine. The procedure: a large-bore needle into the posterior iliac crest of the patient's hip, suctioning out marrow under local anesthesia. The aspirate contains a mix of cells, including a small fraction of mesenchymal stem cells.
This is your own tissue, processed and returned to you. It cannot be rejected. It does not raise donor-matching concerns. It is the safest source on paper.
The yield problem
Bone marrow aspirate is rich in cells overall but sparse in MSCs specifically. A standard pull yields perhaps 10 million nucleated cells, of which only a fraction of a percent are mesenchymal stem cells. Without significant in-lab expansion, the MSC dose from a single bone marrow harvest is a small fraction of what a typical cord-derived dose contains.
Clinics that offer bone-marrow-derived therapy without expansion are giving a substantially lower MSC dose than clinics that use expanded cord cells. Whether that lower dose is clinically meaningful for a given condition is a real question, but it's not the same therapy.
The age problem
Bone marrow MSCs from a 70-year-old donor (yourself, at 70) are 70-year-old cells. They have accumulated 70 years of mutation, environmental stress, and replicative aging. They expand poorly in culture. They produce fewer growth factors and signaling molecules. They senesce sooner.
The cells are as old as the donor.
For older patients, bone marrow as a source has structural disadvantages that no clinic can fix.
The harvest procedure
Bone marrow harvest is invasive. The patient is sedated or anesthetized. Soreness at the puncture site is normal. Bruising is normal. Recovery from the harvest itself is typically a few days. Compared to receiving donor cells via IV. where the patient experiences nothing on harvest because nothing is being harvested from them, bone marrow involves real procedural burden.
For many U.S. clinics, this entire harvest happens the same day as treatment: morning harvest, afternoon injection, no real lab time in between. The result is a minimally manipulated autologous product (legally important under FDA same-surgical-procedure exemption) but a much smaller and less characterized dose than what a full manufacturing pipeline produces.
Adipose tissue, higher yield than marrow, still autologous.
Adipose-derived stem cells (ADSCs) come from a mini-liposuction harvest. A clinician aspirates a small volume of subcutaneous fat (typically 50-200 mL) under local anesthesia, processes the lipoaspirate to isolate the stromal vascular fraction, and either uses the resulting cells directly or expands them in culture.
Yield comparison
Adipose tissue contains substantially more MSCs per gram than bone marrow. A typical fat harvest yields more usable cells than a typical bone marrow pull. For autologous protocols, fat is generally the higher-yield option.
The same caveats
Fat-derived MSCs are still your cells. They are still your age. They still have accumulated whatever environmental stress and replicative aging your tissues have accumulated. The age disadvantage compared to cord MSCs is the same.
And the harvest is still a procedure. Liposuction has real recovery: soreness, swelling, bruising at the harvest sites. For a patient already managing a chronic condition, adding a same-day surgical harvest to the treatment plan is a meaningful additional burden.
The FDA same-day pathway
In the U.S., the most common form of adipose stem cell therapy is "stromal vascular fraction". a minimally manipulated fat extract administered the same day. This operates under an FDA exception for autologous tissue transferred during the same surgical procedure. It allows U.S. clinics to legally offer a stem cell therapy without going through a full IND or BLA pathway: but it also constrains the therapy: no significant expansion, no batch testing, no characterized dose, no consistent product across patients.
How they compare, across the things that matter.
Your own cells, same-day
- No rejection risk by definition
- No donor matching concerns
- FDA same-surgical-procedure pathway in the U.S.
- Low yield: 1–10 million MSCs per harvest
- Cells are your age, older donors, older cells
- Requires a procedural harvest (needle or liposuction)
- Limited expansion; no real batch characterization
- High variability, each patient is their own batch
Donor cells, manufactured, characterized
- Newborn cells, youngest available, highest proliferative capacity
- No procedural harvest on the patient
- Hundreds of millions of cells per batch after expansion
- Full donor screening and tissue testing
- Standardized characterization and potency across all patients
- Requires cGMP manufacturing infrastructure
- Requires international setting in most cases (U.S. regulatory constraints)
- Rare immune response (MSCs are immunoprivileged, but not invisible)
Which source goes where, and why.
Most serious international cGMP programs use cord-derived allogeneic cells for the biological reasons. Most U.S. clinics that operate without manufacturing infrastructure use autologous cells for the regulatory reasons. The choice of source reflects the operating model.
How the physician team chooses.
Celva's physician team at Hospital Angeles, Tijuana does not use a single cell product across all patients. Source, biology, and mechanism expression are matched to the indication, delivery route, and clinical goal. Three allogeneic cell types are in routine use, each one carrying a different profile.
All three are manufactured in our own cGMP lab at Hospital Angeles, operated by Celva's medical team, using proprietary culture media, expansion methods, and protocols developed in-house and used nowhere else. Most clinics don't manufacture at all; whether in Tijuana or Cancún, they buy frozen vials from a third-party lab. Every batch of ours is fully characterized: identity, viability, sterility, mycoplasma, endotoxin, secretome profile. The lab work is the same; the cell type that ends up in the dose is the clinical decision.
Cell type 01 · Umbilical-cord MSCs (UC-MSCs)
Donated umbilical-cord tissue following full-term healthy births. Cells with high proliferative capacity and a robust secretome, higher anti-inflammatory cytokine expression, stronger immunomodulatory activity, greater paracrine output per cell than adult-derived cells. The preferred choice for systemic, neurologic, and autoimmune indications where broad immune and inflammatory recalibration is the primary goal. All four primary mechanisms are active. More on the four mechanisms.
Cell type 02 · Bone marrow MSCs, adult allogeneic (BM-MSCs)
Adult allogeneic donors. Bone marrow aspirate, expanded under cGMP conditions, screened and characterized to the same identity standards as UC-MSCs. BM-MSCs are more lineage-committed than UC-MSCs, biased toward musculoskeletal tissue types. Their cytokine profile includes higher expression of factors associated with tissue remodeling and extracellular matrix support. Preferred for orthopedic and structural environments where particularly strong anti-fibrotic and pro-angiogenic activity is needed to interrupt the fibrotic cascade in chronically inflamed joints and restore vascular supply.
Cell type 03 · Chondrocytes
Chondrocyte-lineage cells, allogeneic, no harvest required from the patient. Chondrocytes are the primary cellular residents of cartilage tissue. Unlike MSCs (which act primarily through paracrine signaling), chondrocytes are structurally oriented. They produce the collagen and proteoglycan matrix that forms cartilage. In depleted or damaged cartilage environments, they provide matrix-building capacity that MSCs alone cannot replicate. Added alongside BM-MSCs in select cartilage cases: knee and hip cartilage degeneration (Grade 2–3 OA), meniscal support protocols, combination orthopedic protocols. Whether structural recovery occurs depends on the patient's tissue environment; the physician team evaluates this carefully. Not all orthopedic cases qualify.
How the call gets made
Cell selection is a clinical decision made during physician-team review, not a product the patient picks at intake. The factors that drive it: the target tissue and its biological environment, which of the four mechanisms needs to be most strongly expressed for the indication, the delivery route (IV for systemic mechanism expression; injection for localized), whether structural support is indicated alongside signaling (the chondrocyte question), and the condition's severity and evidence base. In many cases, a combination protocol (UC-MSCs systemically plus BM-MSCs and chondrocytes at the target site) produces a more complete response than any single cell type alone.
This is also why the program operates internationally. The full manufacturing pipeline (allogeneic expansion, batch characterization, indication-specific selection) requires regulatory and laboratory infrastructure that is not currently available under the U.S. same-day autologous pathway. More on the FDA line.