
The story,
on the day.
A production and editing reference for the patient story film, shot wherever the story lives. Internal & partner use.
One framework. Any patient. Any place.
The production and editing reference for Celva’s patient story film. A two-part format: a short day-of-treatment shoot (1–3 hours), plus a follow-up session 1–6 months later, when results have had time to show.
The structure, scenes, and editing stay the same. Only the patient, the place, and the moment change.
The book pairs with the Celva Brand Guidelines, which covers how the brand looks and sounds. This one covers how we tell the patient’s story.
Two shoots. Two deliveries. One story.
Day-of treatment (1–3 hours): pain, decision, the experience itself. Follow-up (1–6 months later): the actual outcome, captured in person if the patient returns to Mexico, or remotely via video call. The film ships in two phases: a Phase 1 cut from day-of footage (live immediately, no outcome) and a Phase 2 cut after the follow-up. Vendors quote the two phases separately.
Read before every shoot.
Read Chapters 1 through 4 before any new shoot. The principles do not change patient to patient or place to place.
Reference on set.
The question bank, shot list, and timing strip are designed for day-of phone reference. Skim. Pick what fits.
Use as the editing template.
The 6-scene structure and cutdown timelines are the spine of every hero cut.
Seven chapters. One working manual.
Front to back covers everything from why we’re making the film, through the six scenes, to the pre-lock review checklist. The middle chapters (the six scenes, compliance, and the question bank) are the ones you will return to most often.
The patient is the hero. The clinic is the guide.
Two books shape this guide. Campbell gives us the shape. Miller gives us the discipline.
Joseph Campbell
The Hero with a Thousand Faces, 1949
Every hero story shares one shape: call, refusal, threshold, trial, return. The patient is the hero. Their pain is the call. Celva is the threshold. The treatment is the trial.
Donald Miller
Building a StoryBrand, 2017
A hero with a problem meets a guide who gives them a plan. The brand’s fatal mistake is casting itself as the hero. We never do. Celva is the guide. The CTA is an invitation, not a promise.
A short documentary, not a testimonial.
The viewer is not shopping for a clinic. They are someone in pain, scrolling. The first five seconds must make them think “that sounds like me.” Or they scroll past.
What this film is
- A real story, told in the patient’s own voice.
- Story-first. B-roll as proof, not decoration.
- Honest and human. Imperfection is a feature.
- A mini-documentary, not a testimonial.
- The real setting answers skepticism without selling.
What this film is not
- A hard-sell testimonial that opens on a logo.
- A sterile explainer of how stem cells work.
- An outcome-claim piece. No cures. No before/after.
- A doctor-introduction video or a facility tour.
- A B-roll montage over voiceover. The patient must always speak.
The north-star check
Before any cut leaves the bay, ask: Will a viewer think “that sounds like me” in the first five seconds? If not, strip a layer.
The shape of the story.
Five stages compressed into a 3-minute cut. In reality, the journey takes months. The film bridges day-of footage with follow-up footage to deliver the full arc.
“That sounds like me. I have been dealing with the same thing.”
“I have tried everything. No one is giving me real answers.”
“What if there is another option? But is this legit?”
“They actually take care of people. This looks real.”
“They got their life back. Maybe I can too.”
Three acts. Three energies.
Pacing follows the arc, not the runtime. Music supports the patient’s state. Never leads it.
Cuts follow emotion.
Act 1: fast cuts on pain words. Act 2: hold the setting longer as trust builds. Act 3: calm and reflective.
Sparse, warm, restrained.
Open on solo piano or low strings, unresolved. Warm at the decision. Calm through treatment, never triumphant. The patient’s voice is the final sound.
Cinematic. Cool grade.
Wide ratio (2.39:1 letterboxed). Cool teal/ink grade. No on-screen text in the first 8 seconds. Let the patient’s face do the work.
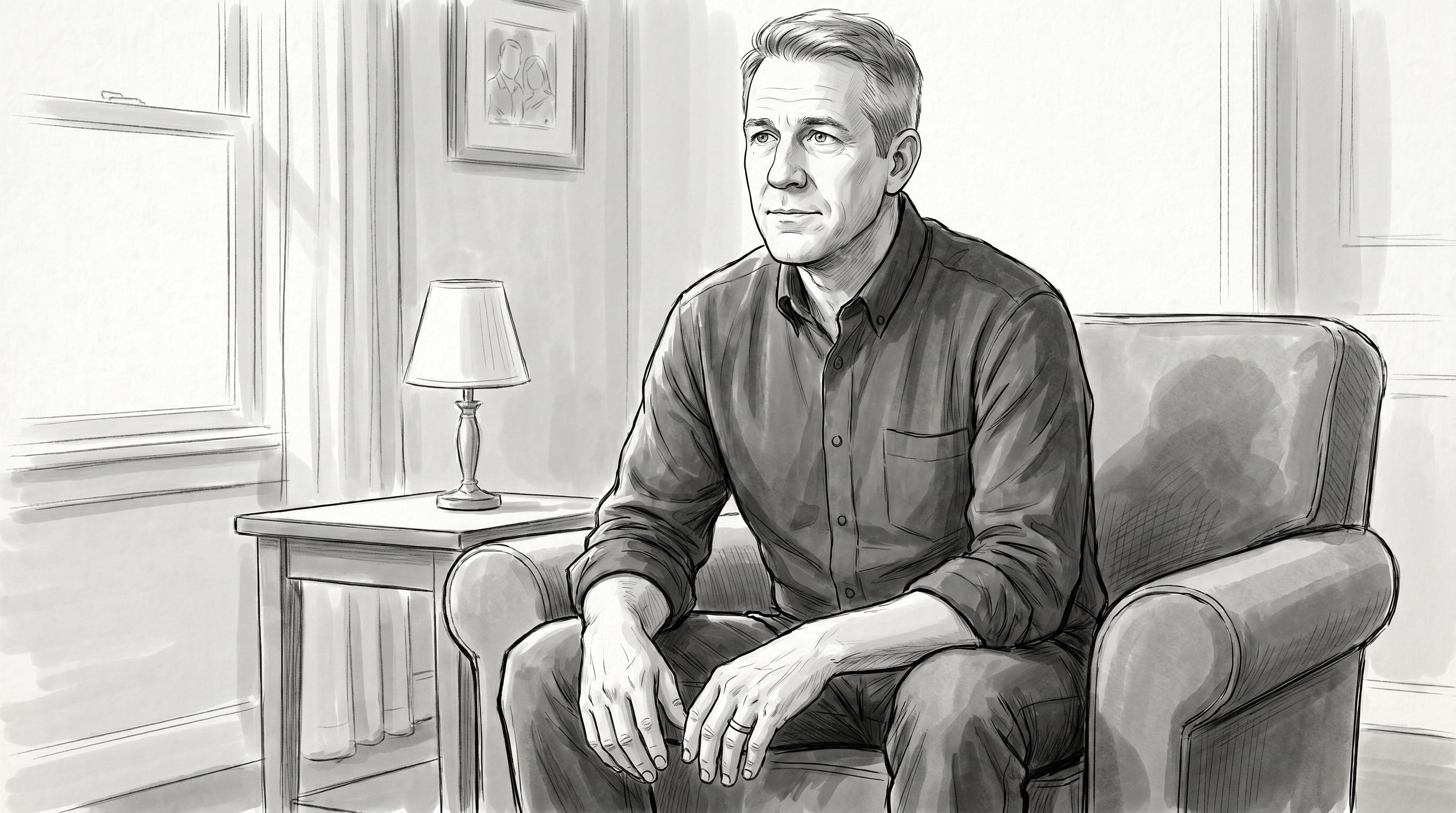
The first five seconds are the entire film.
Do not open on the clinic, the logo, or a building. Open on the patient’s pain, in their voice, with their face on camera.
“I had been dealing with serious knee pain for years, and they told me surgery was my only option.”
“I had really just gotten used to it. I thought this was just how I was going to live.”

Story job
Create the “that sounds like me” reaction. Open on a tight, emotional fragment pulled from Interview 1.
Must capture
- Tight face shot, patient mid-sentence
- Hand resting on the affected area
- Slow walk through a familiar space
- Quiet moment before the experience begins
Audio priority
One raw vocal line describing pain or fear. Breathing, room tone, a single piano note. No music swell yet.
Build like a trailer. Quick fragments. No answers yet. The treatment setting does not appear. We are still in the patient’s old life.
Story job
Let the viewer feel what the patient has lost: work, family, the things they used to enjoy. Establish: they have tried things, none worked.
Must capture
- Patient settled for the interview, speaking
- Empty workout gear, family photos on phone
- Slow movements; hand on the affected area
- Avoid procedural / medical B-roll here
Audio priority
Patient on the emotional cost. Specific people. Specific lost activities.
Nail the pain here and the audience stays. Music sparse. No treatment imagery yet. Not earned.
Story job
First reveal of the place where the experience happens. When at the clinic, the hospital itself begins answering the viewer’s skepticism. The energy shifts from frustration to forward motion.
Must capture
- Slow reveal of the setting (wide)
- Soft focus on patient’s face
- Hands settled, at rest
- Care team or supporting cast in background
- At the clinic: IV line in soft focus, doctor or nurse passing through
- At the clinic: imaging review (MRI scans on a screen, doctor talking the patient through)
Audio priority
Some version of “I knew I needed to do something.” How they found Celva. What made this feel different.
The pivot. Hold the wide of the setting a beat longer than feels necessary. The audience exhales here.
Story job
Pay off the journey. Human care, not medical procedure. At the clinic, the doctors, the IV, the gloved hands. These are the proof of the place.
Must capture
- Process detail: a tool, a measurement, a careful hand
- A caregiver checking in; a smile, no pose
- Patient’s face in repose: calm, half-smile
- Two human-care moments minimum
- At the clinic: vitals, BP cuff, IV drip close-up (no labels)
- At the clinic: imaging machines in frame (MRI, fluoroscope, ultrasound, image-guided injection)
Audio priority
Natural dialogue: “How are you feeling?” “Any questions?” Candid exchanges sell it. Patient voiceover from Interview 1 describes the experience.
Do not over-medicalize. No labels or paperwork in frame. Music warm, calm, never dramatic. Slow the cuts.
Story job
Mark the time gap. Stem cells take months to show. A brief on-screen card and bridging visuals carry the audience from treatment day to the new chapter.
Must capture
- Wide of the patient walking out of the setting
- A title card: “3 months later” or similar
- Quick B-roll cuts from the follow-up footage
- Calendar, seasons, sky: anything that reads as time
Audio priority
Music does the bridge work. A single warm phrase rises here, carrying the audience across the gap. No voiceover yet. The patient’s outcome reveal is held for Scene 6.
This scene is short. 15–30 seconds at most. Its only job is to land that time has passed. Avoid filler. The next scene does the heavy lifting.
Story job
Land the transformation. The patient reflects on what changed, in their own words, with months of real life behind them. Invitation, not promise.
Must capture
- Clean talking head, natural light, calm
- Patient living their life: B-roll specific to what they got back
- Closing one-word or one-sentence summary
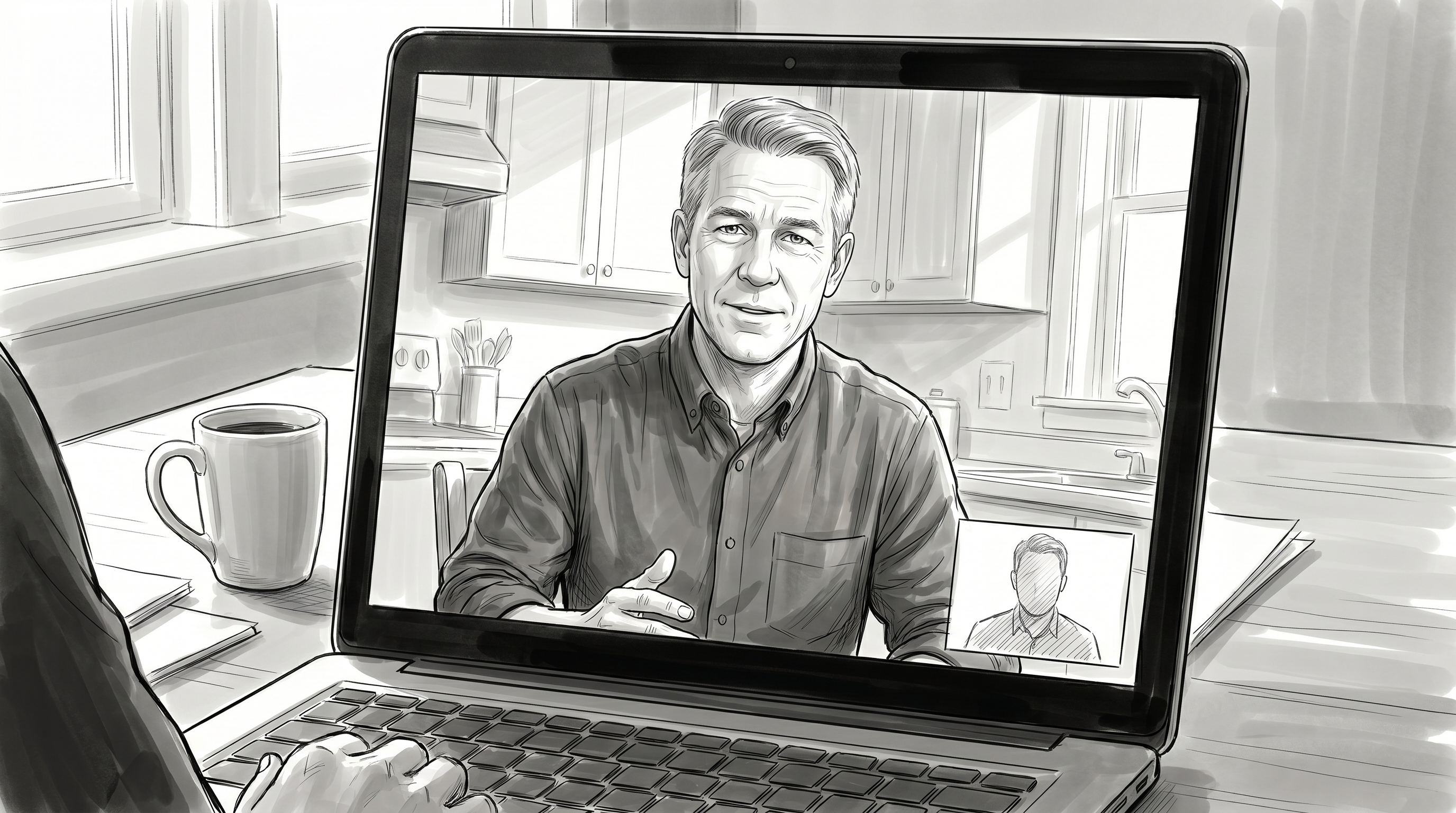
- In person: wider establishing shots of where they are
- Remote: screen of the video call from interviewer’s POV
Audio priority
One clean closing line. Capture two versions: one warm for the hero cut, one tight for cutdowns. Invites a consult; never promises an outcome.
End on emotional clarity, not pressure. The patient’s voice is the final sound. CTA: “book a consult.” Never “get this treatment.”
How the patient is briefed shapes the film.
A cold patient gives short answers. A briefed one gives emotional answers in full sentences. Brief them before each shoot, day-of and follow-up. Same playbook each time.
A short, friendly email.
A 5-minute off-camera sit.
The single most important rule of the shoot day.
Patients default to short conversational answers. Coach them gently into complete emotional sentences. The viewer never hears our questions, only the patient.
How to explain it to the patient
“The people watching this will not hear our voices, only yours. So when I ask what was the pain like?, begin your answer with the phrase the pain was, so it makes sense on its own. Don’t worry if you mess up. We can always re-ask.”
A friend across a coffee table.
The videographer is not a director. Speak softly. Match the patient’s energy. Let pauses happen. The best moments come when the patient stops to find a more honest answer.
Do not cut.
Hold the silence. Those takes go into the final edit. If the camera goes down, the moment is gone. Quiet validation keeps the patient open.
Words and claims that cannot appear in the film.
Not in patient audio. Not in on-screen text. Not in staff dialogue. If a word from the list below survives, the cut is wrong.
Things that cannot appear in frame.
If any of these appears in a shot, the shot does not survive. If it is in frame, reshoot.
Once in the first 20s. Once on the end card.
3 seconds minimum, on screen, legible.
DM Sans 500, 14pt+, navy on white.
Lower-third or full-screen. Not over a face.
Patient redirect, in the moment.
The patient cannot make outcome claims. They can describe their experience. If they cross the line, redirect gently.
The in-the-moment redirect
Do not interrupt mid-sentence. Wait for the breath, then warmly: “That’s wonderful. Can you tell me what you’ve personally noticed?” The patient is the author. We frame; we never edit.
Questions organized by what we want to pull out.
A set of extraction tools, organized by the five emotional outcomes. Outcomes 01–03 are captured day-of, before treatment. Outcomes 04–05 are captured at the follow-up, 1–6 months later, when there is something real to reflect on.
How to use the chapter
Reference, not checklist. Pick what fits. Ask conversationally. Two passes on the most important questions: one clean, one looser. The fill-in-the-blanks are the safety net.
The pain.
What life looked like. What they had to give up.
Watch for: what we want to hear
Specific lost activities (golf, gardening, sleep). Specific people (kids, spouse). A time scale that lands. One short line of fear, in their voice.
If they drift
If they jump to relief, redirect: “Take me back to before today. What was the worst part?”
The stuck.
Tried everything. Doctors had no good answers. The system has failed them.
Watch for: what we want to hear
Failed attempts (PT, injections, meds). A doctor quote. Honest exhaustion. The word stuck, or a synonym, in their voice.
If they drift
If they defend prior doctors, let them. Then: “But how were you feeling about your options?” Bring it back to emotion, not history.
The decision.
Why they acted. How they found Celva. What made this option feel different.
Watch for: what we want to hear
The phrase “I knew I needed to do something” in some form. How they found us. What hesitation looked like: gold for defusing viewer skepticism.
If they drift
If they say “Celva is the best,” redirect: “What made you choose them?” A reason works; a superlative does not.
The relief.
What it felt like to start getting better. Captured at the follow-up, when there is something real to describe.
Watch for: what we want to hear
A specific return (golf, sleep, walking the dog). A specific person who noticed. “Easier than I expected” in some form. Personal experience, never absolute outcome.
If they drift
If they say “I’m cured” or similar, redirect: “Can you tell me what you’ve personally noticed?”
The hope.
What they got back. What they’d tell someone in their shoes today, with results behind them.
Ask the patient to complete each sentence as a complete thought. These are your cold-open and 5-second-cutdown safety net.
“Before I came here, I was dealing with ______”
“The hardest part was ______”
“I was worried that ______”
“I felt like my only option was ______”
“What surprised me most was ______”
“The team here made me feel ______”
“Right now, I feel ______”
“I’m excited to get back to ______”
A small kit. A quiet footprint.
The patient comes first. Gear is sized to disappear into the moment. Not dominate it. Two cameras, two mics, soft light.
Camera · A + B
Two bodies. One mood.
- A-camera: full-frame, 35mm or 50mm prime, for interviews
- B-camera: smaller mirrorless body, 24–70mm zoom, for B-roll
- Gimbal or stabilizer for walking and transitional B-roll
- Tripod for both interview setups
Audio
Two lavs. One shotgun.
- Wireless lavalier · patient
- Wireless lavalier · videographer (reference)
- Shotgun on A-camera as backup + room tone
- Field recorder for ambient sound at each location
- For remote follow-up: screen-record the call; ask patient to record their own audio locally
Lighting
Soft. Augment, never overpower.
- Soft LED panel for the first interview
- Reflector or bounce for the second interview (use natural light primarily)
- Avoid hard lighting that creates clinical shadows
- Keep everything soft and warm
The footprint rule
If a piece of gear cannot fit through the door without disturbing the room, leave it in the case. The patient’s comfort beats any production preference.
The shot list. By location.
The day-of shot list. Capture all of this before wrapping. Re-shoots are expensive and rarely possible. The follow-up has its own shot list (page 28).






Two shoots, two day-strips.
The day of treatment runs 1–2 hours, kept tight. The follow-up runs shorter, 1–6 months later. Both flex around the patient’s comfort.
Find the cold open. Then build everything else.
The cold open (day-of) and closing line (follow-up) are the two emotional anchors. Find them first, then assemble the middle from both shoots.
Find the cold open.
Listen to all day-of interview audio. Pick the strongest 5–7 second emotional fragment. Short. About pain or fear, not the clinic. Works without context.
Find the closing line.
Pull the strongest closing soundbite from the follow-up shoot. The one-word or one-sentence summary. If they gave one word, use it. Closing words are the most-shared line.
Build the audio spine.
Lay interview audio in scene order. Trim aggressively. Read the cut as audio only. Does it travel from pain to hope? Then layer visuals.
Layer the visuals.
Interview footage on emotional beats. B-roll for context. Fast cuts on tension (Scenes 1 + 2). Hold longer on trust (Scenes 3 + 4).
Two deliveries. Multiple cuts.
Day-of footage ships as a complete Phase 1 cut before the follow-up. After the follow-up, the project extends into a Phase 2 final cut with outcome footage. Vendors quote the two phases separately.
Phase 1 · Day-of delivery · ships 2–4 weeks after shoot
Hero, 1:30–2:00.
Phase 1 · Social cut · 30–60s
Phase 2 · Final delivery · ships after follow-up
Hero, 2:30–3:30.
Phase 2 · Social cut · 60–90s + vertical teaser 15–30s
Before the cut leaves the bay.
Every hero edit must clear these before sign-off. If any line cannot be ticked, the cut is not done.
“That sounds like me.”
If a viewer thinks this in the first five seconds, the film works. If not, nothing else matters.
In doubt? Reach out.
If a question is not answered here, it’s a missing page. Tell us; we’ll write it.